NRNP 6645 Family Assessment and Psychotherapeutic Approaches Paper
NRNP 6645 Family Assessment and Psychotherapeutic Approaches Paper
Walden University NRNP – 6645 Psychotherapy with Multiple Modalities
Family Assessment and Psychotherapeutic Approaches Historian: Mother and daughter (Self)
Language: English
Name: Non- listed
Gender: Both female (mother and daughter)
Age: 40 years old and 23 years old.

Chief complaint — “I am in so much pain, nobody can help me and nothing is helping me manage the pain. I want my mom to be more peaceful, I want her to lower her expectations and accept a lot of things about life, I have a sense that my mom is holding me back from all I could be doing”. I just want them to spend time with me, I am very lonely, and I get depressed when I am lonely. I hate spending time with my mother, I hate her house, she has two dogs and I do not like those at all, I do not like their hair on my body and I do not like touching them. Do you believe I cannot even eat in her house, everything smells like dog, and it is very uncomfortable for me”.
History of present illness (HPI) — This patient is a 40-year-old Iranian American female. She is here today to be seen for complex family dynamic issues as it relates to her and her five children. She was seen with her 23-year-old daughter who detailed the multiple issues as it relates to her relationship with her mom and siblings. They are here for evaluation of trauma related issues as it relates to abuse by her husband and their father. Mom is currently struggling with trauma related issues from being married and also struggling with adjusting to the norms and principles of America which can be called Adjustment disorder at this time
Per self report, one of her daughters was raped and abused by her biological father and this has left a dent in the way the family relates with their dad. There has been difficulties relating to one another, difficulties relating to their father, difficulties relating to the issues of traditional Iranian family becoming “Americanized”, issues with spending time with their mother, their lack of privacy and distrust overall.
Overall, this is a complex family unit and there are multiple conflicts active and ongoing at the same time. The biggest issue has to do with the mother of the house becoming sick, and having multiple surgeries to fix her foot which has left her almost dependent. The second issue is the rape allegation. One of the daughters alleged that her biological father raped her., this has left the family traumatized and unforgiving.
Thirdly, there is the issue of the of a mother desperately trying to hold unto her traditional Iranian beliefs and traditions. For example, in Africa and the Middle East, it is believed that children are to stop their lives to care for their parents if they need that help. In America, the tradition is to employ a capable nursing facility or a private nurse to do the caring. These are very different standards. In this case, her children are urging her to do more for herself and for her health, to not solely depend on them or wait on them. Overall, there are major unresolved conflicts going on that are trauma related, depression, physical health etc.
Some physical signs noted during the assessments were fidgeting, excited. There are also signs of hyperactivity, impulsivity, irritability, lack of restraint, and persistent repetition of words. There is no notice of difficulty focusing, issues with paying attention or short attention span.
Past psychiatric history — In the scenario, mom mentioned depressive episodes, there was however no mention of medically diagnosed psychiatric conditions like depression. They denied suicidal ideations. They also denied the use of illicit drugs/ alcohol, prior serious mental or psychiatric breakdown, or mania. No prior reports of psychiatric inpatient hospitalizations to report either.
Hospitalizations- No inpatient psychiatric hospitalizations reported nor are there any reports for active Pyschotherapy medications listed for these patients.
Psychotherapy or previous psychiatric diagnosis — No current psychiatric diagnosis, no Psychotherapy “therapy” is documented for this patient. Note however that the patient said she “gets depressed when she is alone”. It was not reported that depression was medically diagnosed or that it is currently being managed by any medication.
Pertinent substance use- Patients deny alcohol or abusing any substances at this time.
They also deny any chronic substance use/abuse.
Family psychiatric/substance use– Patients deny any family psychiatric/ substance use.
Psychosocial history/Developmental history — These patients are 40 and 23-year-old Iranian immigrants that are currently struggling with adjusting their traditional beliefs with the Americanized way of life. They are here today for mental assessment/ possible diagnosis of trauma related issues including adjustment disorder. They were referred by their current psychiatrist who has tried multiple dimensions to manage the patient and her children. Of note, she was present for the assessment and answered pertinent questions as it relates to the patients, their past and their overall issues.
Mom is currently living on disability but her daughter that came with her for the evaluation lives by herself. Of note, it was reported that she is currently in school, but her social life was not discussed during assessment. It is always vital to know your patients, for this evaluation., there was no concrete data collected or reported. For example, knowing what school the daughter attends, her sexual orientation, understanding her full social life is important in treatment plan.
Questions like does she have a boyfriend and does she live with him? Is she bisexual? What kind of friends does she have? How many drinks does she drink during nights out? What kind of alcoholic beverages does she drink? Collecting, collating and analyzing these informations can create a well-rounded scenario and can help in creating a full treatment plan for targeted intervention.
Knowing our patient’s lifestyle and if they indulge in high risk behaviors can assist in creating a plan of care that can address the specifics for high risk behaviors like testing periodically for STDs, liver functions, and sometimes suicide. As we all know, alcohol and drug use can contribute to unintentional injuries and sometimes violence. Tobacco use, unhealthy dietary behaviors, physical inactivity and sexual behaviors can all contribute to unintended pregnancy and sexually transmitted infections. It is therefore imperative to assess these functions and tailor care to fit the assessment (Kelley, T., 2016)
For these patients and the family as a whole, there was no mention of past or current medical history. From what I could deduce from the assessment, mom recently had surgery of her bilateral foot. The reason for this surgery or what prompted it was not reported. To understand this patients whole health history, it is imperative to ask some vital questions.
Considering her physical weight, I would want to know is she diabetic? Does she suffer from hypertension? What medications does she take daily to manage these ailments? These are vital information because we would know how to vigorously manage her wounds and how well she may heal after surgery. (Kelley, T., 2016). Unmanaged diabetes can lead to necrotic wounds that may not heal which can lead to sepsis. It is therefore vital to have a clear picture of your patient during assessment (Kelley, T., 2016)
Work History — None on file/ assessed
Legal history — None on file/ assessed
Medical History– No head injuries to report, no seizures, no developmental concerns.
Current Medications– None listed
Allergies — Unknown
Medical Diagnoses — none listed
Reproductive Hx — Post 6 children for mom, unknown for the children.Relationship
— Mom is separated from her husband and the father of her children, no relationship status posted or reported for her children
Educational Level — None listed for everyone involved in this assessment
Occupation — None listed or reported
Hospitalizations — None reported or found in the chart.
Family Medical History —None reported or assessed from previous visits
Review of Systems (ROS)
General– mom reports fatigue and tiredness, denies night sweats, fevers, chills. Daughter reports being fine but just overwhelmed by her moms demands and unaware of how to manage the situation.
HEENT– No visible head injuries or trauma noticed on both patients, patients deny change in vision, hearing, no ear pain, blurred or double vision, or yellow sclerae. Ears, Nose, Throat: No hearing loss, sneezing, congestion, runny nose, or sore throat
Skin — No skin issues or concerns to report or noted.
Cardiovascular — No chest pain, heart palpitations, syncope, or edema noted on both patients.
Respiratory — No cough, wheeze, or diminished breathe sounds noted, occasional dyspnea with exertion noted, perhaps related to anxiety and depression.
Gastrointestinal — No abdominal pain, constipation, diarrhea, nausea, constipation. No anorexia noted.
Genitourinary — No flank pain, dysuria, burning on urination, hematuria etc.
Musculoskeletal — No myalgias, no joint pain.
Hematologic — No anemia. No easy bruising or bleeding.
Lymphatics — No lymph nodes issues to report. No enlarged nodes. No history of splenectomy.
Endocrinology — No diabetes, no thyroid disorders. No polyuria, polyphagia, or polydipsia, or polyphagia.
Neurological — No headaches, dizziness, syncope, paralysis, ataxia, numbness, or tingling in the extremities. No change in bowel or bladder control.
Physical Exam (Done by PCP)
T- 98.3 R 16 106/72 Ht 5’7 Wt 117lbs
Average build
Vital signs
RR:16 bpm, BP: 106/72, O2: 98%
Temp — 98.3 F,
P– 69
Weight — 117 lbs.
Height — 5’7, and 5’11 respectively
Head — atraumatic
Eyes — white sclera bilaterally, pink conjunctiva
Ears — patent, no discharge, grey pearl TM bilaterally.
Nose — pink mucosal membranes bilaterally, no congestion and intact turbinates
Throat — red mucosal membrane. No exudates.
Neck — no swelling and bruits. ROM is full.
Lungs — symmetrical chest, symmetry in expansion, and resonant sound in all areas. Cardiovascular — S1, S2 clear, and no murmurs. Peripheral pulses 3+ and no edema. Abdomen — flat and symmetrical, no tenderness, no masses, & normoactive sounds Musculoskeletal — 5/5, no disuse/atrophy/hypertrophy.
Neuro — intact from CN I up to XII
Lymph/skin — no edema, no swelling.
Mental Status Examination
Mom is a 40-year-old Iranian female and her daughter is a 23 Americanized Iranian female. Mom looks older than her stated age perhaps due to stress from being married young and in an abusive marriage. Her daughter here today looks her stated age with no concerns. He is cooperative with the examiner. They are both neatly groomed and clean, they are also dressed appropriately for the weather and times. There is no evidence of any abnormal motor activity., They both however present with significant anxiety, restlessness and irritation. They deny any visual or auditory hallucinations, delusions, tangentiality/mood. Their speeches are clear, stressed and loud but coherent and normal in volume and tone. Thought process is goal driven and logical.
There is clear evidence of annoyance, excitability, fidgeting, hyperactivity, impulsivity, irritability, medium restraint and persistent repetition of some words in a forced and aggressive tone. They seemed present-minded when spoken to, there is no difficulty focusing, no lack of memory recall/ forgetfulness, no issues paying attention, and no issues with short attention span. Their moods are gloomy and affect is appropriate to presented moods (flat). They deny any auditory or visual hallucinations. They also deny any current suicidal or homicidal ideations.
Cognitively, they are alert and oriented to themselves, the situation and recent and remote memories are intact. Concentration is normal, insight is average, there is no difficulty in memories recollection. Abstraction, attention, insight, and judgment are all reasonable and intact.
Eye contact– Good
Speech — Normal rate and volume. Behavior — Anxious (for both patients) Psychomotor — No involuntary movements. Mood — gloomy
Affect — Flat.
Thought Process: logical, goal-directed and organized.
Thought Content: no delusions. — no suicidal ideations, — no homicidal, or self-harm ideations noted.
Perception: Minimum reaction to external stimuli.
Attention/ Concentration: Sustained attention and concentration observed.
Cognition: Alert, and oriented X 4. Memory: No issues with recall Insight: Fair.
Judgment: Average
Fund of Knowledge: Average. Intelligence: Average
Post Traumatic Stress Disorder Diagnosis and Screening in Adults.
Previously, PTSD was simply called a “soldier’s heart,” “shell shock,” or “combat fatigue.” The terminology of post-traumatic stress disorder (PTSD) arose immediately after the Vietnam War. It was observed that traumatic events lead to a complex psychobiological presentation during and after the Civil War (Patra, B. N.,2018).
This disorder was first described by ABR Myers (1838–1921) in 1870, it was described as a multifaceted disorder with complex factors and presentation combining acute fatigue, dyspnea, a sighing respiration, palpitation, sweating, tremor, an aching sensation in the left pericardium, utter fatigue, an exaggeration of symptoms upon efforts and in severe cases syncope that can happen suddenly (Iribarren, J., 2015).
Differential Diagnoses
POST- TRAUMATIC STRESS DISORDER- PTSD; ICD-10 CODE: F.43
PTSD can occur after a traumatic event such as military combat, a violent physical assault, or a natural disaster. While stress is usual after a trauma, people with PTSD often relive traumatic events in their minds countless times. They may also begin to feel distant from friends and family. They may also start to experience various emotions and experience anger that does not go away over time, or perhaps even get worse.
This disorder usually affect individuals who have experienced a wide range of life- threatening occurrences. According to research, approximately 8% of the American population will experience PTSD at some point in their lives. In Veterans, PTSD is commonly associated with combat trauma. According to the National Center for PTSD, the prevalence of PTSD is not fixed on race, sexual orientation or physical features, it can happen to both men and women in various capacities.
The stress that results from traumatic events bring about a spectrum of psycho-emotional and physiopathological consequences. Post-traumatic stress disorder (PTSD) is a psychiatric disorder that expresses itself as a result of an experience or of a witnessing of really traumatic or a life-threatening episode. Post Traumatic Stress Disorder has a profound psychological correlation with generalised physical impairments. These symptoms can profoundly impair an individual’s daily life functions and can be life and mind-altering. This disorder is common in extended combat, terrorism, exposure to certain environmental toxins etc. Overall, per recent research, there is expected to be a rise in individuals with Post Traumatic Stress Disorder diagnosis is expected in upcoming decades
Overall post-traumatic stress disorder (PTSD) is a disorder that develops in certain individuals who have experienced a shocking, scary, and or a dangerous experience that has left scars too fearful to forget. As we all know, fear triggers many split-second changes in the body to help defend against danger scenarios and propel certain actions that it deems fit would cause rescue from the situation. This episode known simply as “fight-or-flight” response is a typical reaction meant to shield an individual from harm in frightful circumstances.
Of note., 95% of individuals will experience a variety of reactions after a life- altering trauma episode, but most people will recover fully from initial symptoms without any external help or re-direction. The individuals who keep experiencing trauma as a result of an experience will be diagnosed with PTSD. People who have this disorder usually feel stressed or frightened, even when there is no danger lucking around.
All criteria met : Some signs of PTSD are persistent thoughts about a past event, persistent negative emotional thoughts, extreme thoughts of fear, fear, horror, anger, guilt, or shame. “Markedly diminished interest or participation in significant activities” (Adler et al., 2006; Glind et al., 2013). These patients are currently experiencing chronic signs of PTSD, from being married to an abusive man and from having a sister that was sexually abused by their father.
Another significant factor of PTSD verbal aggression, unsanitary home, and economically depressed lifestyle. These factors are current in “moms” behaviour. Her verbal aggression has also contributed significantly to her estrangement from her children.
ADJUSTMENT DISORDER — ICD-10-CM Code F31
Adjustment disorder refers to an unexpected strong behavioral or emotional reaction that occurs as a result of an identifiable stressful life change or that occurred within the past three months. It can present in multiple forms and behaviors, these can include the feeling of hopelessness, sadness or persistent stress. This can also include physical symptoms occurring after one undergoes through a stressful event in life. Overall, adjustment disorder primarily deals with mood, while acute stress disorder deals with environmental stimulation (Harvard Medical School, 2017). Psychological symptoms such as anxiety, low mood, irritability, emotional ups and downs, poor sleep, poor concentration, wanting to be alone etc are some symptoms.
Fundamental issues coping with daily activities, mental abilities and general day-to-day activities are some challenges of having this disorder.
As at the time of this assignment, there is no known cause of this disorder.(Brüne, 2015). However, the disorder is thought to be as a result of life’s stressors and experiences, interaction of genetics, temperament and altered levels of some chemicals in the brain. Over the years, research has revealed that certain events can increase the chances of developing this disorder.
These events can range from daily challenges to school functions. In the psychiatry community, there is a belief that genetics is again believed to play a significant role in the formation, while the environment is assumed to play an aggravating factor in its activation and symmetry. Overall, a combination of genetics, the environment, and sometimes a “modified” brain structure and chemistry may play a significant role.
Significantly, management for this disorder can be lifelong and treatment revolves around intricate combination of medications, psychotherapy and other kinds of therapies. Psychiatric Mental Health Nurse Practitioners diagnose Adjustment disorders after reviewing the patient’s symptoms, overall history, life experiences plus family history etc. As we all understand in Mental illnesses, it is vital to diagnose adjustment disorders early enough for a targeted intervention and expected outcome to occur promptly.
“The Outcome of Depression International Network (ODIN) project shows adjustment disorder in less than 1% of population. Another recent study of the general population found the prevalence of adjustment disorder to be about 0.9%. Note that when the criterion of clinically significant impairment was considered. A further 1.4% of the sample was diagnosed with adjustment disorder without fulfilling the impairment criterion” (Patra, B. N., 2018).
All criteria not met: The diagnostic criteria is not met due to the time frame for the diagnosis which ranges between 0-3 months. Some symptoms of adjustment disorder are feeling sad, hopelessness or lack of enjoyment. Adjustment disorders do share some symptoms with depression and some Practitioners have diagnosed depression in place if this disorder. Frequent crying, worrying or feeling anxious, nervous, jittery or stressed out, trouble sleeping, lack of appetite, difficulty concentrating, feeling overwhelmed, and lastly difficulty functioning overall (Ustun, B., 2017)
ACUTE STRESS DISORDER— 2021 Acute Stress Disorder DSM-5 308.3 (F43.0)
Acute Stress Disorder (ASD), unlike Adjustment disorder, develops within the first month after an individual develops/ witnesses an event that involves a threat or actual death. Overall, these patients respond to these events with excessive feelings of helplessness, dread and horror. ASD was introduced as a diagnostic procedure to help in identifying persons that would ultimately develop post-traumatic stress disorder (PTSD). However, PTSD and ASD differ in two major ways (Brüne, 2015).
The obvious difference between ASD and PTSD is the onset and duration of symptoms. The effects of ASD present immediately and last up to a month, while PTSD symptoms present slower and last longer, up to several years if not treated. Psychological symptoms such as anxiety, low mood, irritability, emotional ups and downs, poor sleep, poor concentration, wanting to be alone are all signs and symptoms that point to ASD.
All Criterias not meet;- Based on the accepted time frame for diagnosing this ailment, it is highly impossible for these patients to be suffering from acute stress disorder. This is a possibility but not a diagnosis at this time. PTSD as a result of a traumatic marriage and abuse is the more possible choice at this time.
Case Formulation and Treatment Plan
The main treatments for people with PTSD are medications, psychotherapy, or both. Everyone is different, and PTSD affects people differently, so a treatment that works for one person may be ineffective for another. It is important for patients with PTSD to be managed by a licensed mental health provider that is experienced and knowledgeable with this disorder. Some people with PTSD may need to try different treatments to find what works for their symptoms. This is where an experienced practitioner comes in.
The complicating factor in mental heath is the factor of co-occuring mental illnesses. It is vital to treat illnesses from their root course. For example, if my patient is going through PTSD as a result of an abusive and physical relationship, it is important to stop that trigger and that may usually mean ending the relationship and charting a new course of rehabilitation. Like I pointed out prior, if depression is related to the root cause of a patients PTSD presentation, that depression has to be treated with first class SSRI and psychotherapy, or possibly group therapy depending on the trigger and aggravating factor. Other ongoing problems that can co-occur are panic disorder, depression, substance abuse, and suicidal ideation.
Mom in this scenario is exhibiting signs and symptoms of socialization skills and has noticed an increase in her depressive issues. Linkage to community resources, assistance with medical appointments, psychotherapy, and problem-solving with issues related to activities of daily living.
Treatment Plan
Prozac 20mg daily Buspar 15mg BID Seroquel 50mg po QHS
Psychotherapy with Cognitive Behaviour Therapy to be followed up in four weeks.
Stress management
Diet and Nutrition specialist
Medications side effects and overall expectations.
Reflections /Legal and Ethical Implications
As I began to study the scenario and the topics for this assignment, I was intrigued by the spectrum and the many factors that set each mental illness factor apart. PTSD is a complex disorder that most folks incorrectly relate to veterans. Many neurotransmitters are associated in the formation and sustainability of PTSD. So far Glutamate and Dopamine are said to be the largest contributor in this class. The prefrontal cortex is also implicated in the roles in attention and regulation of impulse control in impulse control. EEG studies found elevated beta activity in their electroencephalography studies (Sadock, B. J., 2015).
Considering that patients with PTSD have a predisposition to obesity, it is imperative that these patients understand the detriments of having excess body weight as it predisposes them to acute and chronic illnesses like diabetes mellitus, hyperlipidemia, obstructive sleep apnea, cardiovascular disease, chronic obstruction pulmonary disease, rheumatoid arthritis etc. “Post Traumatic Stress Disorder is associated with an increased risk of type II diabetes mellitus,” (Brüne, 2015 ). Across the lifespan, there is a correlation between PTSD and complex health complications. Including behaviors that can trigger high risk behaviour regardless of their consequences.
Some high risk behaviors that can be activated as a result of PTSD are substance abuse, binge-eating, obesity, and improper/unsafe sexual behavior etc. It is therefore imperative to educate these patients on the importance of safe sex practices, healthy food options and exercises. Practitioners and their patients may discuss healthy habits, healthy meals and exercises with this patient to promote good health and prevent diseases and complications (Sadock, B. J., 2015).
In ethical implications, confidentiality in practice has always been the strongest contender. Mental illness has continued to be a source of stigmatization and mockery in our communities today. It is therefore important to maintain HIPPA laws to the full extent the law permits. Lastly, the principle of autonomy, justice, beneficence, and nonmaleficence must be maintained throughout the interaction with the patient and thereafter. Legal and ethical implications have to be considered during every patient/ provider encounter. Patients and their families must be given accurate and up to date information, and given the options to either seek care or decline.
NRNP 6645 Family Assessment and Psychotherapeutic Approaches Paper References
- “Mother and Daughter: A Cultural Tale.” , directed by Anonymous., Masterswork Productions, 2003. Alexander Street, https://video.alexanderstreet.com/watch/mother-and- daughter-a-cultural-tale.
- Sadock, B. J., Sadock, V. A., & Ruiz, P. (2015). Kaplan & Sadock’s synopsis of psychiatry (11th ed.). Wolters Kluwer.
- American Psychiatric Association. (2013). In Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596.dsm05
- Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
- Rajan P. (2017). Community physiotherapy or community-based physiotherapy. Health promotion perspectives, 7(2), 50–51. https://doi.org/10.15171/hpp.2017.10
- Patra, B. N., & Sarkar, S. (2018). Adjustment disorder: current diagnostic status. Indian journal of psychological medicine, 35(1), 4–9. https://doi.org/10.4103/0253-7176.112193
- Brüne, M. (2015) Textbook of Evolutionary Psychiatry and Psychosomatic Medicine: The Origins of Psychopathology. OUP Oxford. http://www.ptsd.va.gov/professional/treatment/early/acute-stress-disorder.asp
- Iribarren, J., Prolo, P., Neagos, N., & Chiappelli, F. (2015). Post-traumatic stress disorder: evidence-based research for the third millennium. Evidence-based complementary and alternative medicine : eCAM, 2(4), 503–512. https://doi.org/10.1093/ecam/neh127
- Kelley, T., Docherty, S., & Brandon, D. (2016). Information needed to support knowing the patient. ANS. Advances in nursing science, 36(4), 351–363. https://doi.org/10.1097/ANS.0000000000000006
Family Assessment and Psychotherapeutic Approaches
Different families have different family dynamics. This paper discusses the case of a 40-year-old Irani mother who immigrates to the United States with her children. Patti has five children: Sheela, age 24; Sharleen, age 23; Shireen, age 21; Armin Jr., age 18; and Sam, age 15. Shireen has recently been reunited with her family after her mother immigrated to America and left her in Iran with her father. Patti reports to the clinic because there has been chaos at home since her daughter rejoined the family after 10 years.
The chaos began two weeks ago when Shireen started reporting how her father emotionally, physically, and sexually abused her. She blames her mother for this. She felt abandoned. The history also reveals that Patti has had surgery on both her feet. Patti lives at home with her two sons. Shireen got married secretly and moved out. The other daughters live on their own. Patti has increasingly felt lonely and helpless. She wants her daughters to stay at home or visit more often. Her daughters feel that they want Patti to practice independence as they also have their lives to live.
Differential diagnosis
Post-traumatic stress disorder. (PTSD) is a mental disorder that occurs after someone close to them is exposed to an extremely threatening or horrifying event. An example would be physical trauma or sexual trauma in childhood. The patient may have a delayed presentation of symptoms. A diagnosis can be made in patients who have had an impaired function for one month. The criteria for diagnosis include persistent intrusive memories, recurrent distressing dreams, prolonged psychological distress, avoidance of reminders and stimuli, self-blame or blame of others, feelings of estrangement and detachment from others, persistent negative emotions such as anger and guilt, self-destructive behavior, and angry outbursts (Herringa, 2017).
Both Patti and Shireen most likely have PTSD. They meet a number of the criteria required to diagnose this disorder. Patti was married to an abusive husband. She says she would step in between her husband and her children to protect them. When she left Shireen in Iran, she was worried that Shireen would have no one to protect her from the abuse. She is also concerned that her daughters may get married to an abusive husband. Ever since Shireen reported the trauma she endured at the hands of her father, the house has become an uncomfortable place. Patti feels guilty for what Shireen went through. Shireen blames her mother for all her trauma. Patti says that she enjoyed that quiet that came after Shireen left.
Adjustment disorder is an impaired emotional or behavioral response to change or a stressful event. The symptoms usually consist of stress that is out of proportion to the expected reaction. The reaction can also cause an impairment in daily functioning. The DSM-5 criteria for adjustment disorder include onset of behavioral symptoms within three months of an identifiable stressor. The distress is disproportionate to the stressor with cultural and contextual factors considered. The symptoms should cause impairment in daily functioning. The symptoms should also not meet the criteria for other mental disorders.
The symptoms should not last for more than six months after the exposure to the stressor or resolution to a stressor (O’Donnell et al., 2019). The aftermath of Patti’s surgery is that she has chronic pain and is now disabled. This has affected her independence, and this causes stress and tension at home as she depends on her children more. She wants her daughters to stay at home or visit more often and be around more. Patti might be having an adjustment disorder. She has not come to terms with the fact that her daughters are grown and need to have their own lives. She demands too much of their time, and her daughters feel like Patti is overdependent. She also tries to impose the Iranian culture on her children. She doesn’t want to accept that the way of life in America might be different from the one she grew up in, which is Iran.
Acute stress disorder (ASD) is a disorder that is an acute stress reaction that occurs between three days and four weeks after a traumatic event. The risk factors for PTSD could also lead to ASD. Factors such as the female gender, history of traumatic events, assault, and rape are all risk factors. The DSM-5 criteria for ASD include exposure to a traumatic event, recurrent distressing memories of the traumatic event, and flashbacks of the traumatic events. Other criteria include a negative mood, dissociative symptoms, arousal symptoms, and avoidance symptoms. The difference between ASD and PTSD is the onset of symptoms (Bryant, 2018). Patti and Shireen are unlikely to be suffering from ASD based on the onset of symptoms for ASD.
Plan of Care
A treatment plan is meant to help a patient achieve their objectives. The treatment plan consists of Psychotherapy using cognitive behavioral therapy (CBT) to help with PTSD. This should focus on increasing knowledge of trauma psychology. Patients should be taught ways to identify and dispute thoughts that cause them to relieve the trauma (Schrader & Ross, 2021). Family therapy is also necessary to help resolve the chaos and tension in the family. Patti and Sharleen should continue with family therapy.
Family therapy would provide a platform for them to air their issues with a therapist acting as the moderator. Both parties can find a middle ground where they can both agree. The rest of the family members should also be encouraged to join the sessions. Shireen, who was sexually abused, should be educated on the importance of therapy. Her mother reports that she declines therapy and prefers that she is given the money used in therapy instead. Family therapy focuses on individual family members’ emotions and helps resolve them. Unresolved emotions can lead to frustrations in the family.
A multicultural framework should be employed when handling the cultural differences between Patti and her children. Patti should understand that her children are more used to the American culture. Some practices that may be perceived as radical in Iran are considered conservative in America. Patti’s children feel suffocated. Patti should also be educated on the importance of letting her daughters live independent lives.
Patti should be made aware of the different ways of living. She should understand that this is another country and that the children will eventually need to grow on their own. Patti should be made aware that there are other ways in which she might get resources.
Patti has chronic pain and should therefore have a prescription for analgesics. Patti should also be educated on the benefits of exercise on weight loss. She should be encouraged to exercise and observe a heart-healthy diet. A diet and nutrition specialist should be consulted to help formulate an appropriate diet.
Genogram
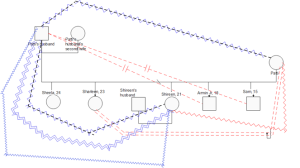
Patti’s husband physically abused Patty. She reports a history of battering and domestic violence. Patti and her husband are separated. Patti’s husband has remarried. Shireen was emotionally, physically, and sexually abused by her father. Ever since the abuse on Shireen came to light, Armin and Sam want nothing to do with their father. They are estranged. Sharleen and her mother have a tense relationship. Sharleen feels like her mother suffocates them. She is torn between taking care of her mother and moving on with her life. She feels stuck. Patti has a distant relationship with Shireen.
References
Bryant R. A. (2018). The Current Evidence for Acute Stress Disorder. Current Psychiatry Reports, 20(12), 111. https://doi.org/10.1007/s11920-018-0976-x
Herringa R. J. (2017). Trauma, PTSD, and the Developing Brain. Current Psychiatry Reports, 19(10), 69. https://doi.org/10.1007/s11920-017-0825-3
Mother and Daughter: A Cultural Tale. (2003). [Video/DVD] Masterswork Productions. https://video.alexanderstreet.com/watch/mother-and-daughter-a-cultural-tale
O’Donnell, M. L., Agathos, J. A., Metcalf, O., Gibson, K., & Lau, W. (2019). Adjustment Disorder: Current Developments and Future Directions. International Journal Of Environmental Research And Public Health, 16(14), 2537. https://doi.org/10.3390/ijerph16142537
Schrader, C., & Ross, A. (2021). A Review of PTSD and Current Treatment Strategies. Missouri Medicine, 118(6), 546–551.
Also Read: Captain of the Ship Project – Obsessive Compulsive Disorders Paper