Summary and Descriptive Statistics Paper
Summary and Descriptive Statistics Paper
From the descriptive, the Black and white communities, including the Hispanics record the highest means at 69.5 and 62.3 for each sample of 100, 000 people respectively. On the other hand, the lowest means are recoded by the Pacific Islanders including Hispanic and Asians of any race at 38.29 and 31.31 respectively. This indicates that cancer rates is highest among the black and white communities and lowest among the Pacific islanders and Hispanics.

Then again, the variance reflects the deviation of the data from the mean. The highest variance is recorded among the American Indian including Hispanics Black and white communities at 29.6, 44.1 and 29.2 respectively. The variance suggests that the number of year-to year cases among these communities have the highest variation. By contrast, the variance of the Asian, and Hispanics is the lowest, which indicates that the changes in the cancer cases recorded annually vary slightly from one year to another among these communities.
Instructions for Summary and Descriptive Statistics Paper
There is often the requirement to evaluate descriptive statistics for data within the organization or for health care information. Every year the National Cancer Institute collects and publishes data based on patient demographics. Understanding differences between the groups based upon the collected data often informs health care professionals towards research, treatment options, or patient education.
Using the data on the \”National Cancer Institute Data\” Excel spreadsheet, calculate the descriptive statistics indicated below for each of the Race/Ethnicity groups. Refer to your textbook and the Topic Materials, as needed, for assistance in with creating Excel formulas.
Provide the following descriptive statistics:
Measures of Central Tendency: Mean, Median, and Mode
Measures of Variation: Variance, Standard Deviation, and Range (a formula is not needed for Range).
Once the data is calculated, provide a 150-250 word analysis of the descriptive statistics on the spreadsheet. This should include differences and health outcomes between groups.
All documents needed to complete this assignment will be uploaded.
| American Indian / Alaska Native (includes Hispanic) | Asian / Pacific Islander (includes Hispanic) | Black (includes Hispanic) | Hispanic (any race) | White (includes Hispanic) | National Cancer Institute (2018) Lung and bronchus cancer. Retrieved from Janary 8, 2019 from https://seer. | |||||||||
| Year of Diagnosis | Rate per 100,000 | Rate per 100,000 | Rate per 100,000 | Rate per 100,000 | Rate per 100,000 | |||||||||
| 2000 | 45.7 | 41.8 | 77.8 | 34.2 | 68.8 | |||||||||
| 2001 | 47.9 | 41 | 79 | 34.1 | 68.7 | |||||||||
| 2002 | 44.6 | 40.4 | 75.8 | 34.1 | 68 | |||||||||
| 2003 | 50 | 40.9 | 77.3 | 34.5 | 67.1 | |||||||||
| 2004 | 51.7 | 40.5 | 75.1 | 35 | 65.8 | |||||||||
| 2005 | 48.7 | 40.2 | 73.7 | 33.8 | 65.9 | |||||||||
| 2006 | 46.4 | 39.8 | 73.4 | 32 | 65.8 | |||||||||
| 2007 | 43.1 | 38.8 | 71.2 | 32.7 | 65.2 | |||||||||
| 2008 | 45 | 38.5 | 70.8 | 32.2 | 63.9 | |||||||||
| 2009 | 40.1 | 39 | 71.6 | 31.8 | 63.1 | |||||||||
| 2010 | 42.4 | 37 | 67.8 | 30.3 | 60.4 | |||||||||
| 2011 | 39.6 | 36.6 | 64.1 | 29.4 | 58.5 | |||||||||
| 2012 | 36.6 | 36.7 | 64.3 | 28.2 | 57.5 | |||||||||
| 2013 | 39.9 | 36.6 | 60.5 | 28.8 | 56.3 | |||||||||
| 2014 | 32 | 34 | 61.3 | 26.8 | 55.4 | |||||||||
| 2015 | 38.7 | 34.4 | 57.4 | 26 | 53.2 | |||||||||
Analyzing Descriptive Statistics
Descriptive statistics means interpreting data sets from a particular population or sample to derive meaning, summarize, or understand outcomes (Kaliyadan & Kulkarni, 2019). As a DNP-prepared nurse, it is essential to have the skills in analysis, understanding, and interpreting statistical data in quantitative research and, therefore, be able to apply statistical analysis in practice change projects (Jones et al., 2021). This discussion presents an analysis of descriptive statistics on a rural clinic’s practice change project on DSME and the interpretation of the project’s outcome based on the dataset acquired pre and post-intervention.
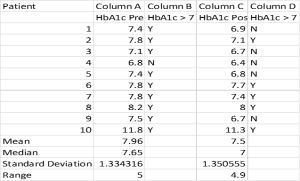
Based on the dataset provided in the table above, the following calculations were made
- Percentage of patients with Uncontrolled diabetes pre-implementation and Post Implementation
Pre-implementation 90%
Post-implementation 50%
- Mean of the HbA1c pre-implementation and post-implementation
Pre-implementation 7.96
Post-implementation 7.5
- Median Scores, Pre-implementation, and Post-Implementation
Pre-implementation 7.65
Post-implementation 7
- Pre-implementation and Post-Implementation Standard deviation levels
Pre-implementation 1.33
Post-implementation 1.35
- Pre-Implementation and Post-Implementation Range
Pre-implementation 5
Post-implementation 4.9
Descriptive Analysis Statistics
The measures of central tendency before the intervention implementation were mean 7.96, median 7.65, standard deviation 1.33, and range 5. Post-implementation measures were Mean 7.5, Median 7, standard deviation of 1.35, and a Range 4.9. 90% of the diabetes patients involved in the intervention implementation had uncontrolled diabetes HbA1c greater than 7% at the project’s beginning, but the percentage decreased to 50% by the end of the implementation, showing a difference of 40%.
The practice change project, therefore, demonstrates an improvement in the HbA1C levels of the patients involved since the average HbA1c levels reduced from 7.96 to 7.5 after the implementation of the intervention. The measures of central tendency calculated above show that the variability in the data set is large. However, the abnormal range could have been caused by the outlier on patient #10.
After implementing the change project, the mean of the HbA1c levels dropped from 7.96 to 7.5, showing an improvement in the efficacy of better glucose level management, thus improving HbA1c control. The percentage of patients who had uncontrolled HbA1c levels also dropped from 90%-50%, thus improvement in diabetes management and control. However, the data set shows that patient #10 HbA1c levels are an outlier. Amrhein et al. (2019) note that an outlier in a data set influences the understanding of the data. Similarly, it has affected the understanding and deriving conclusions from the data since it has caused an increase in the range, median, and mean, which is not the actual population representation.
Conclusion
The descriptive statistics analysis has demonstrated an improvement in the control of glucose levels for the patients after the implementation, thus showing success. Based on these results, I would recommend continuing the intervention since it has improved overall diabetes control. I would also recommend implementing the intervention for other diabetes patients in the institution and other institutions since it has demonstrated success.
Summary and Descriptive Statistics Paper References
Amrhein, V., Trafimow, D., & Greenland, S. (2019). Inferential statistics as descriptive statistics: There is no replication crisis if we do not expect replication. The American Statistician, 73(sup1), 262-270 https://doi.org/10.1080/00031305.2018.1543137
Jones, M., DeValpine, M., McDonald, M., & Schubert, C. (2021). Use of statistical tests in Doctor of Nursing Practice projects. The Journal for Nurse Practitioners, 17(9), 1118-1121. https://doi.org/10.1016/j.nurpra.2021.06.006
Kaliyadan, F., & Kulkarni, V. (2019). Types of Variables, Descriptive Statistics, and Sample Size. Indian Dermatology Online Journal, 10(1), 82–86. https://doi.org/10.4103/idoj.IDOJ_468_18
HLT 362 Week 4 Quality Improvement Proposal Paper
Healthcare practice is faced with various problems from time to time. These problems may impact the provision of good care quality, patient outcomes, and organizational performance. However, these practice problems and issues are good opportunities for quality improvement. Healthcare leaders are tasked with initiating quality improvement opportunities and implementing them based on the evidence-based practice process, thus addressing the issue and improving patient outcomes and organizational performance.
One of the quality improvement opportunities in my practice is the high cases of catheter-acquired urinary tract infections. Therefore, the quality improvement project is a clinician education program focusing on addressing catheter-acquired urinary tract infections. This paper describes catheter-acquired urinary tract infections and a quality improvement project proposal on the issue.
Problem and Setting Overview
Catheter-acquired urinary tract infections (CAUTI), also known as catheter-associated UTIs, are infections in the urinary tract in which the positive culture is taken when an indwelling urinary catheter has been in place for more than two calendar days. Patients with indwelling catheters in the bladder are predisposed to UTIs and are susceptible to bacteria in the urine since the catheter is a foreign substance to the bladder.
Additionally, the catheter inserted acts as an initiation site for infections due to the introduction of foreign bodies into the urinary tract. CAUTI infections affect any part of the urinary system, including the bladder, ureter, urethra, and kidneys. Catheter-acquired urinary tract infections are the most reported hospital-associated infections in the National Healthcare Safety Network. According to the Centers for Disease Control and Prevention (n.d.), approximately 75% of urinary tract infections acquired in hospitals are associated with catheters. Therefore, catheter-associated urinary tract infections are a severe problem in hospital settings.
Quality Improvement Initiative Justification/Expected Outcomes
All healthcare institutions aim to deliver care services that produce desirable outcomes and optimal quality. Providing quality healthcare services entails ensuring patient safety, the effectiveness of care, patient-centeredness, efficiency, timelessness, and equity. Healthcare institutions put in place various measures and tools to ensure quality, assess performance, and notice areas of quality improvement (Quentin et al., 2019).
Additionally, patient safety is one of the measures of care quality. The primary patient safety concerns that raise questions about care quality include hospital-acquired infections. As mentioned earlier, the most frequently reported hospital-acquired infection is catheter-acquired urinary tract infections, despite being highly preventable. Therefore, initiatives to prevent cases of CAUTI are necessary.
Furthermore, CAUTI negatively impacts the patient’s health outcomes. According to Ladhani et al. (2020), CAUTI is usually associated with other complications, including sepsis and bacteremia, which may turn, lead to death, prolonged hospitalization, and increased cost burden for the patient and the healthcare system. More so, 15-25% of hospitalized patients receive urinary catheters during their hospital stay, showing that a considerable population is predisposed to the risk of CAUTI (CDC, n.d.).
Hence, the quality improvement initiative on clinician education will improve quality and performance outcomes for the healthcare institution and patient outcomes. The expected project outcome is improved self-reported knowledge and confidence in CAUTI s management and prevention, which will translate to decreased prevalence of CAUTI and a reduction of mortality cases related to CAUTI.
Research Evidence Supporting the Proposed QI Initiative and Projected Outcomes
According to Reynolds et al. (2022), quality improvement initiatives using multifaceted interventions to reduce the prevalence and incidence of catheter-acquired urinary tract infections, especially in intensive care units, have effectively ensured a sustained reduction of CAUTI cases. Successful quality improvement interventions addressing CAUTI concerns include education, cognitive aids, and real-time feedback on patient care quality. The intervention outcomes are reduced urine culture rates, reduced catheter utilization, and decreased CAUTI incidence rates (Reynolds et al., 2022).
Furthermore, multidisciplinary teams-led QI initiatives on CAUTI have been found to considerably reduce the cases of CAUTI across different care institutions. A study by Ramakrishna et al. (2022) shows an improvement in infection prevention following reduced cases of inappropriate catheter insertions and prolonged removals. The outcomes resulted from implementing a quality improvement intervention that focused on care provider education (for doctors and registered nurses) and the design and implementation of appropriate urinary catheter practice algorithms. The initiative improved the confidence and knowledge of the care providers in the prevention, management, and control of catheter-associated urinary tract infections in the study.
Research shows that various catheter practice algorithms and urinary tract assessment tools have been developed to prevent CAUTI (Narula et al., 2019). However, most interdisciplinary team members are unaware of these evidence-based practices, and thus the need for clinician education to create awareness and improve knowledge and practices on CAUTI prevention, management, and control. Narula et al. (2019) note that education interventions can be used to create awareness of CAUTI prevention and management best practices, thus helping reduce the incidence of cases and improve patient safety and health outcomes.
From the research evidence presented above, the use of clinician education, specifically focusing on nurses and physicians as a QI initiative for CAUTI, is effective in leading to positive outcomes. The positive outcomes indicated in the research include increased knowledge and confidence in CAUTI prevention and management and reduced CAUTI incidence and prevalence.
Steps of Implementing the Quality Improvement Initiative
When implementing a quality improvement initiative, it is critical to identify a model that can be used as a framework to guide the implementation, assess the progress and obtain feedback for continuous improvement (Livesay, Zonsius & McNett, 2022). The model that will be used in this quality improvement initiative is the six sigma model. The six sigma model eliminates defects and errors in procedures and processes. The model mainly has two methodologies; Define, Measure, Analyze, Design, Verify (DMADV), which is used when developing a product from scratch, and the Define, Measure, Analyze, Improve, Control (DMAIC), which is used for the improvement of already existing procedures and processes. DMAIC is the most used model for quality improvement initiatives in healthcare.
The first step in this process is defining the project goals. The project goals are defined by identifying what needs to be accomplished, the people who should be involved in accomplishing the goal, and galvanizing the resources and support needed. In this case, the project goal is to conduct clinician education on nurses and physicians concerning the prevention, management, and control of catheter-associated urinary tract infections.
The project will involve various stakeholders, including healthcare leaders, nursing managers from different units, nurses, physicians, and an external educator- a specialist in infection control and CAUTI prevention and management. Support from the healthcare institution leaders is also essential in this project. The project team will hold a meeting with the leaders and develop a presentation to explain to them the existence and intensity of the problem, thus garnering their support for the initiative. The resources needed include financial resources, educational materials, space, and time for conducting the clinician education program.
The second step is the measure. It involves measuring the performance of the existing process when it is unaltered. My healthcare institution uses a CAUTI best practice algorithm to control and manage CAUTI. In this step, the current intervention, which is the use of algorithms, will be measured on its effectiveness based on its purpose.
The third step is to analyze. The step entails an analysis of the possible causes of the current problem. The current process or measure is analyzed to identify the root causes resulting in the defects. In this case, the use of CAUTI best practice algorithms will be assessed to identify what could be the root cause of increased catheter-acquired urinary tract infection prevalence and incidence.
The fourth stage, improvement, involves addressing the problem, given that its root causes have already been identified. The changes that can be implemented to address the problem are modified into a plan of action for improving the condition and contributing to change. The fifth and final stage of the process is the control stage. The stage entails continuous monitoring and evaluation of the process while incorporating feedback learned from tracking the progress. Evaluation of the initiative at this phase would determine whether the improvement initiative has met the set outcomes, that is, increased knowledge and self-reported confidence among care providers on the prevention, control, and management of CAUTI.
Evaluation of the Quality Improvement Initiative
Evaluation of quality improvement initiatives assessing whether the project led to the desired outcomes and to what extent the project implementation the quality improvement project improved efficiency and effectiveness in the issue of concern (Livesay et al., 2019). There are various ways in which quality improvement initiatives are evaluated. In this case, the quality improvement initiative will be evaluated based on three improvement aspects; the acceptance and adherence to the revised practices, the extent to which the new practice impacts the delivery of patient-centered care, and the extent to which patient care and experience have improved.
The number of care providers attending the training and the incidence of CAUTI is the measures that will be used to evaluate whether there was an improvement. The variables that would be used to test whether the initiative was successful include clinician education and self-reported confidence in the prevention and management practices of CAUTI. The hypothesis that would be tested to identify the improvement is that clinician education improves self-reported knowledge and confidence in CAUTI prevention and management. The statistical test that can be used is the t-test, which measures changes in a population before and after the intervention. These tests will help identify if the improvement initiative succeeded.
Conclusion
In summary, the issue of concern that is a perfect opportunity for quality improvement is the high incidence and prevalence of CAUTI. The proposed quality improvement initiative is clinician education for nurses and doctors. The projected outcomes include increased self-reported knowledge and confidence in CAUTI prevention/management. The six sigma model will be used in the initiative’s implementation. Evaluation will be done to identify project success.
References
Centers for Disease Control and Prevention (n.d.) Catheter-associated Urinary Tract Infections (CAUTI). Retrieved 17th February 2023 from https://www.cdc.gov/hai/ca_uti/uti.html
Ladhani, H. A., Tseng, E. S., Claridge, J. A., Towe, C. W., & Ho, V. P. (2020). Catheter-Associated Urinary Tract Infections among Trauma Patients: Poor Quality of Care or Marker of Effective Rescue? Surgical Infections, 21(9), 752–759. https://doi.org/10.1089/sur.2019.211
Livesay, S., Zonsius, M., & McNett, M. (2020). Evaluating data to guide care delivery: Quality improvement methods and implementation science. In Data for Nurses (pp. 59–86). Academic Press. https://doi.org/10.1016/B978-0-12-816543-0.00005-4
Narula, N., Lillemoe, H. A., Caudle, A. S., Chemaly, R. F., Anderson, J. J., Segal, C., Porter, C. A., Swisher, S. G., Levenback, C. S. & Aloia, T. A. (2019). Postoperative urinary tract infection quality assessment and improvement: the STOP UTI program and its impact on hospital-wide CAUTI rates. The Joint Commission Journal on Quality and Patient Safety, 45(10), 686–693. https://doi.org/10.1016/j.jcjq.2019.06.001
Quentin, W., Partanen, V.M., Brownwood, I., & Klazinga, N. (2019). Measuring healthcare quality. Improving healthcare quality in Europe: Characteristics, effectiveness, and implementation of different strategies [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK549260/
Ramakrishna, J. M., Schmidt, B., Hessler-Waning, M., Reddy, T., Hester, T., Kashlan, R., Tariq, O., McCready, T. & Tegeltija, V. (2022). 2028. Reduction in Health Care Facility Onset Catheter-Associated Urinary Tract Infections: A Resident-Led Quality Improvement Initiative. In Open Forum Infectious Diseases (Vol. 9, No. Supplement_2, pp. ofac492-1651). US: Oxford University Press. https://doi.org/10.1093/ofid/ofac492.1651
Reynolds, S. S., Sova, C. D., Lewis, S. S., Smith, B. A., Wrenn, R. H., Turner, N. A., & Advani, S. D. (2022). Sustained reduction in catheter-associated urinary tract infections using multifaceted strategies led by champions: A quality improvement initiative. Infection Control and Hospital Epidemiology, 43(7), 925–929. https://doi.org/10.1017/ice.2021.135
Also Read: What Is a Worldview?